

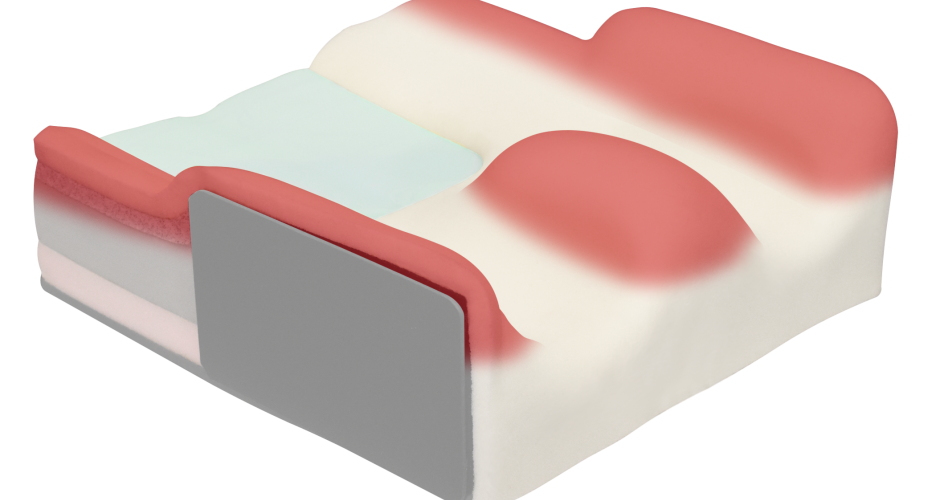
Cushion contouring can provide stability, comfort, and help to offload pressure from the main weight-bearing areas of the buttocks and back of the thighs onto the medial or lateral area. This is achieved by maximising surface contact between cushion and the wheelchair user, maintaining or improving pelvis alignment and body posture and preventing factors that contribute to abnormal tone and pain.
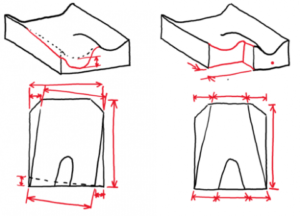
| An ischial well that helps to orientate the pelvis into position at the centre rear of the cushion. This helps to maintain the pelvis directly below the upper body and contributes to avoiding secondary complications such as twisting of the upper body if the pelvis is positioned to one side. This also optimises the alignment of the hips and thighs on the cushion and can reduce secondary complications in the lower body such as wind sweeping of the hips. |  |
| A pre-ischial shelf that may be built in or simply evident within the different foam layers between the ischial well and the forward section of the cushion. This provides support around the curved aspect of the ischial tuberosities, can help to block the ischial tuberosities from migrating forward (e.g. into posterior pelvic tilt) and keeps the pelvis orientated into the ischial well area. This shelf can also help to reduce pelvic rotation, which affects the alignment of the spine and hips in sitting. |  |
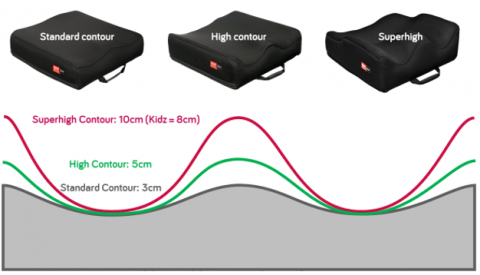
| Contouring under and around the thighs and pelvis which helps the wheelchair user relax into the base of support, maintains the orientation and optimal neutral alignment of the pelvis and thighs on the cushion and increases the surface contact area which increases pressure distribution for comfort and skin integrity. Contouring can also help to resist tendencies to adduct the hips (where the knees touch) in the presence of instability or increase tone. The surface contouring is often available at different heights and the wheelchair user may require increase contouring heights for specific postural needs so that the cushion provides biomechanical support to maintain optimal pelvis and thigh alignment in sitting. |  |
This can be in response to clinical needs relating to pressure, increase/reduced tone, instability, and/or physical discomfort. For example:
Increasing thigh lateral contour heights on one or both sides helps to:
- Block hip abduction and help to maintain a more symmetrical and optimal hip alignment in sitting where the hip joint is free to move or there is a reducible hip abduction towards neutral.
- Provides increase surface contact to the lateral sides of the thigh in addition to the back of the thigh on the cushion surface. This helps with pressure distribution over a larger area and can help to reduce pressure peaks and maintain skin integrity.
- Provide added lateral support to the thigh(s) which can increase the stability on the seating surface to allow for improved trunk, upper limb, and head function.
- Allow the thighs to relax into the cushion to optimise comfort.
Increased medial thigh contour height helps to:
- Provide a biomechanical block to hip adduction in the presence of increased tone or to align the hip into a more neutral alignment in the presence of reducible hip adduction.
- Allow the thighs to assume a more neutral position on the seat and increasing contact surface for a more stable sitting posture
Is the cushion appropriately sized for seat width and seat depth to fit the wheelchair user’s body measurements?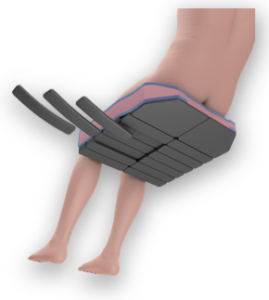
Is it clinically required:
- Has the assessment of factors affecting posture (range of movement, tone, pain, alignment, pressure) indicated this is required?
- Is tone fully understood and addressed? Contouring may need to match the user’s thigh and pelvis position but may also need adjustment if tone presentation varies.
- Are future adjustments to contouring required because of a change in clinical and posture presentation?
- If the pelvis is in posterior tilt, with the bottom perhaps sliding forward on the seat, a higher medial thigh contour may result in increased pressure to the groin and
 genital area. This increase skin integrity concerns and can contribute to pain or additional postural distortions if the user attempts to offload pressure by, for example, rotating the pelvis. Use of a pelvic support belt and considering cushion shaping is recommended to optimise the pelvis position, alignment, and orientation on the seat cushion to avoid this.
genital area. This increase skin integrity concerns and can contribute to pain or additional postural distortions if the user attempts to offload pressure by, for example, rotating the pelvis. Use of a pelvic support belt and considering cushion shaping is recommended to optimise the pelvis position, alignment, and orientation on the seat cushion to avoid this.
 |
 |
There are additional contouring options that are either inherent in cushion selection or require further customisations, which can include:
- Providing a chamfer at the front of the cushion so that the wheelchair user’s feet can be tucked back under the seat. This is often required for wheelchair users that may have shortening of their hamstrings or have increased tone in the flexor muscles of their legs. Failure to accommodate this results in the wheelchair user’s pelvis often being pulled forward on the cushion. This can compromise the support and pressure offloading within the ischial well as well as create posterior pelvic tilt, which creates a hyper kyphosis in the trunk and contributes to secondary postural deformities.
- Shortening the leg length for one leg on the cushion. If the wheelchair user presents with different femoral (thigh) length with one shorter than the other, failing to reduce the cushion depth on the shorter side will result in the cushion depth causing the pelvis to be pulled forward on that side, contributing to rotation and secondary postural deformities in the spine.
- Off setting the standard alignment of contouring for users who have complex postures and need this to be accommodated within the seat cushion e.g. wind sweeping of the hips.
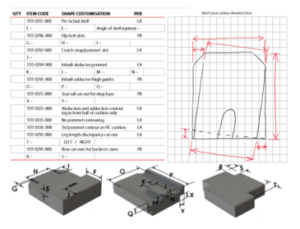
- Shaping the cushion to meet the user’s individual body shape and postural needs by use of surface or strategic positioning base configuration. The Spex Classic Cushion allows this contouring to be provided through the base configuration layers so that the user maintains a consistent contact area with the surface of the cushion for comfort and pressure distribution, whilst also allowing additional customisations to surface contours and shaping, as required.
The Product Performance table below rates some key features of each off-the-shelf cushion using a rating scale of 1-5*.
Spex Vigour Cushion
|
Spex Classic Cushion
|
|
| Pressure Care | 3 | 4 |
| Positioning | 3 | 4 |
| Lateral Stability | 3 | 3 |
| Offloading | 3 | 4 |
| Changing Needs | 1 | 4 |

*Product Performance ratings are used to compare Spex products only.
Please note that additional customisations are available on all Spex cushions to meet the needs of complex wheelchair users and details of how to do this are found on the Spex Build-Your-Own Cushion Script Form available here. For clients with hip range asymmetries please refer to Constructa Flex.
As with all seating solutions and prescription, individual adjustments may be required; each wheelchair user should be adequately assessed with regards to their level of function, assistance needed and postural alignment before deciding on the cushion and the contouring in relation to their defined goals.
If you need any advice on the cushions, please contact us or your local distributor.