


This blog aims to provide some guidance on the potential causes and presentations of tight hamstrings for wheelchair users. Seating solutions will be considered along with how Spex cushions can help to manage outcomes for functional seating.
The hamstrings are not just one muscle but consist of three muscles at the back of the thigh that stretch from the pelvis to the back of the lower leg. They originate from the ischial tuberosities of the pelvis and insert onto the tibia or fibula – the bones below the knee. Each are bi-articular muscles – simply put, this means that they affect movement at two joints: the hip and the knee. The names of these muscles are biceps femoris, semitendinosus and semimembranosus and they are innervated by the Sciatic nerve.
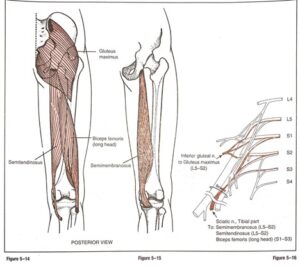
Hislop & Montgomery, 1995, p.176
These muscles are responsible for extension of the hip and flexion (bending) of the knee, and influence rotation of the hip. They work together with the various muscles responsible for the opposite movements (flexion of the hip and extension of the knee). For every muscle that contracts in the body, there is another muscle that stabilises and/or lengthens to allow us to perform smooth, coordinated movement patterns.
When muscle tone is affected it can result in weakness or tightness in the muscle. This, together with any persistent shortening/lengthening of muscles due to neurological and positioning consequences, will reduce ease of movement and affect postural control and coordination.
Tight hamstrings can be considered as an inability or restriction to move easily or fully through their available range of movement.
- Persistent postures where the hamstrings are in a shortened position. Reduction of physical activity and mobilisation, prolonged positioning in bed and poor sitting postures can lead to a reduction of the available stretch and range of movement. This creates tightness because the range of movement is limited.
- Pain can contribute to tensing of the muscles which may appear as tight hamstrings, preventing a person from being able to sufficiently relax onto the cushion with the feet below the knees.
- Instability in sitting can result in a wheelchair user needing to ‘fix’ or stabilise to feel safe and be able to function – we may see wheelchair users actively tucking their legs under the seat or using their legs to maintain contact with the wheelchair frame for additional support It is good to note that, by improving stability within the seating system, we can prevent this adopted posture from potentially developing into long-term hamstring tightness.
- Muscle tone changes from neurological conditions such as a stroke or Cerebral Palsy can result in increased tone within the muscle, reducing the ease of stretching and available range of movement within the muscle. When this affects hip flexion on just one side, it “…increases the odds of pelvic obliquity, trunk asymmetry, scoliosis and windswept hip distortion” (Ágústsson et al, 2017).
- Injury or muscle strain.
Even when full range of movement in the hamstrings may be possible but difficult to maintain because of discomfort or pain, it is best to consider how to optimise functional seating that promotes comfort, stability, and engagement in activities.
Because the hamstrings are biarticular and affect the hip and knee joints we may see limitations in range of movement at one or both. Tight hamstrings may present as a hip flexion limitation, often accompanied by knee extension limitation.
For example:
- Able to bend (flex) the hip sufficiently so that the user can sit on a flat surface, but presenting with the foot tucked under the seat, with difficulty or inability to bring the foot comfortably forward to rest under the knee or forward of the knee. The wheelchair user is likely to have a posterior pelvic tilt which may be exaggerated if the feet are encouraged forward onto footplates.
Waugh & Crane, 2013
- Unable to bend (flex) the hip sufficiently to sit on a flat surface, but the foot is below the knee (e.g., perch sitting where the pelvis is higher than the knee), causing pelvic obliquity and rotation.
Waugh & Crane, 2013
- Flexion limitations at both the hip and the knee that require custom or specialist seating options to accommodate and provide stability.
- Difficulties leaning forward in the seat once seated.
- Difficulty achieving full extension in the knee when performing standing transfers on/off the wheelchair, which may impact the success of pelvic placement on the wheelchair if ability to move on the seat is also impaired – this may result in additional need for caregiver support.
![]()
We want to optimise symmetry for stability, considering each wheelchair user’s unique body shape, range of movement limitations, functional needs, and goals.
Seating provision should always be functional, meaning that it is an “individually driven, guideline-based seating intervention to promote task performance
(Costigan & Light, 2011)
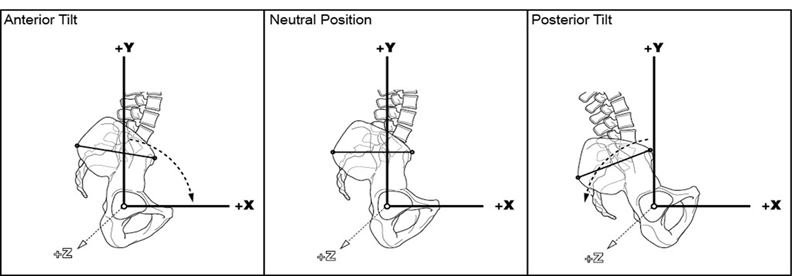
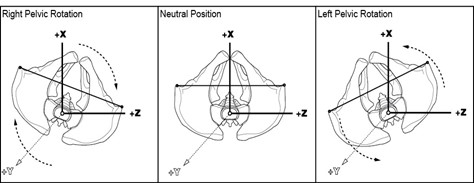
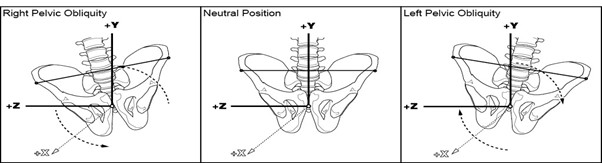
To promote stability and reduce potential secondary complications, wheelchair seating should ideally allow the trunk to remain upright in a vertical position above the pelvis, maintaining the neutral spinal curves; and should allow the head to be stacked vertically above the trunk. The trunk position depends on the position of the pelvis on the cushion, which can be affected by tight hamstrings. The pelvis should be in a neutral resting sitting posture (without posterior or anterior tilt, obliquity, or rotation) and if this is not possible the seating system should optimise stability that is pain-free, least effortful to maintain, and should accommodate limitations to range of movement.
When sitting on a flat surface, tight hamstrings may cause the wheelchair user to move their pelvis forward on the seat so that it now is in front of the trunk on that side (causing pelvic rotation and posterior tilt), as well as potentially causing the pelvis to lift off the seat (obliquity – down on the opposite side) and rotate towards the opposite side from the side with the tight hamstrings. These pelvic positioning changes can lead to secondary postural complications and avoidable postural distortions. We want to control the rotation and obliquity of the pelvis for a good sitting position and we want to prevent pelvic tilt that flattens or exaggerates the spinal curves.

(Left) Possible seating postural presentation due to tight hamstrings and (Right) available accommodation to optimise functional seating on Spex
Considering the hip joint.
- Back support recline:
- Often the wheelchair back support can be adjusted to increase the angle of recline to accommodate limited hip flexion caused by tight hamstrings. This reduces the bending of the hip by opening the seat to a back support angle. This, however, requires careful consideration as it may compromise functional seating and contribute further to postural distortion and discomfort if the wheelchair user must work to hold their head up against gravity. It can result in forward flexion of the trunk and neck (exaggerating the kyphotic curve of the spine) and increased effort if the wheelchair user uses their arms to self-propel. This can lead to fatigue and discomfort for the active wheelchair user. Pressure risk also needs to be considered as there is the potential for increased shear and sacral loading on the cushion if the wheelchair user’s pelvis slides forward on the seat cushion or is not sufficiently stabilised.
- Cushion configuration for limited hip flexion:
- Increasing the height of the pelvis in relation to the knees through cushion configurations maintains an upright trunk but it also allows a more open (extended) hip angle on the same seat without compromising an optimised neutral positioning of the pelvis.
 |
 |
 |
(Left) Example of Spex Classic cushion (Middle & Right) Example of increasing pelvis contouring height to allow right thigh to drop down on the Spex Flex cushion.
- Examples of cushions that offer this include the Spex Classic cushion and the Spex Flex cushion, with the Spex Flex cushion offering support for wheelchair users requiring responsiveness to greater hip flexion limitations (70° – 90°).
Considering both hip and knee joint.
- For particulary tight hamstrings, both the hip and knee angles need to be considered simultaneously. For wheelchair users with a reducible limitation requiring a gradual approach towards a more neutral resting sitting posture, the cushion may need to allow gradual adjustment over time. The Spex Classic cushion and the Spex Flex cushion are designed for this, allowing immediate and gradual adjustment by changing the base pocket-layer and wedge contouring to adjust thigh to trunk and thigh to lower leg angles, respectively.

Example of how the off-the-shelf Spex Flex cushion responds to knee flexion (chamfered front edge), hip flexion limitations and pelvic obliquity.


- Ágústsson, A., Sveinsson, Þ., & Rodby-Bousquet, E. (2017). The effect of asymmetrical limited hip flexion on seating posture, scoliosis and windswept hip distortion. Research in Developmental Disabilities, 71, 18–23. https://doi.org/10.1016/j.ridd.2017.09.019
- Costigan, F. A., & Light, J. (2011). Functional Seating for School-Age Children with Cerebral Palsy: An Evidence-Based Tutorial. Language Speech and Hearing Services in Schools, 42(2), 223. https://doi.org/10.1044/0161-1461(2010/10-0001)
- Hislop, H. J., & Montgomery, J. (1995). Daniels and Worthingham’s Muscle Testing: Techniques of Manual Examination (6th ed.). W.B. Saunders Company.
- Lange, M. L., & Minkel, J. L. (2018). Seating and Wheeled Mobility: A clinical resource guide. Slack Incorporated.
- Miller, F. (2018). Stiff Knee and Knee Extension Deformities in Cerebral Palsy. In F. Miller, S. Bachrach, N. Lennon, & M. O’Neil (Eds.), Cerebral Palsy (pp. 1–12). Springer International Publishing. https://doi.org/10.1007/978-3-319-50592-3_138-1
- Waugh, K., & Crane, B. (2013). A clinical application guide to standardized wheelchair seating measure of the body and seating support surfaces. (Revised). Assistive Technology Partners. https://pva-cdnendpoint.azureedge.net/prod/libraries/media/pva/library/publications/lib_waugh-guide-to-seating-v2-measures-revised-ed-compressed.pdf