


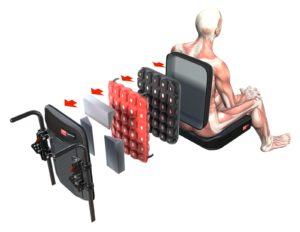
The back support, cushion height and width selection is dependent on a number of factors. The base of the back support generally runs from the height of the posterior superior iliac spines (PSIS) to the chosen height against the user’s back depending on the support needed for stability and the freedom of movement required at the shoulders (e.g. if a wheelchair user is self-propelling).
The cushion and back supports are primary surfaces involved in functional seating and both have a direct effect on sitting posture. This is a two-part blog that explores how the back support can offer biomechanical support to maintain pelvic alignment and stability, particularly in the transverse plane (pelvic rotation) and sagittal planes (posterior/anterior pelvic tilt).
Pelvic rotation means that either the left or right side of the pelvis is more forward on the seat compared to the other. We can easily assess for pelvic rotation by feeling where the anterior superior iliac spines (ASIS) are in relation to the other when in a sitting/lying position and seeing if the posterior iliac crests rest equally on the surface in lying. Pelvic rotation is a crucial axis of movement that needs assessment for wheelchair seating.
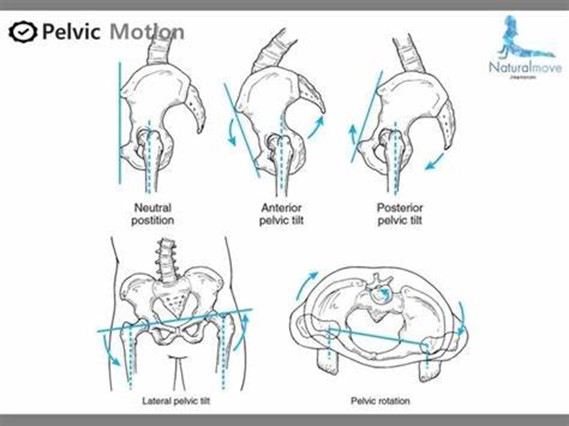
Figure 1 Illustration of pelvis in neutral and with asymmetry (http://blog.naver.com/naturalmove/220534758029)
Let’s consider how a configurable back can be used to respond to the following pelvic presentations, bearing in mind that the cushion must be carefully considered to optimise pelvic stability and alignment also:
Non-reducible pelvic rotation:
- Padding within the back support can be removed on the side of the pelvis that is rotated backwards and built up on the side of the pelvis that is rotated forward.
- This supports and stabilises the pelvic orientation which increases stability of the upper body without aggravation or increasing the rotation already present. An anterior pelvic support device such as a belt, can be used to block migration of the pelvis into further rotation and to provide additional stability.
- By meeting the contours of the body, the back support continues to provide optimal pressure distribution to prevent soft-tissue deformity or further postural asymmetry because of insufficient support and stability being offered.
Figure 2. View from above – Spex Supershape back support shaping in response to pelvic rotation and trunk asymmetry with lateral trunk supports providing additional trunk support.
 |
 |
| Figure 3. Spex Supershape configuration layers | Figure 4 Spex TSS for added contouring behind contouring foam back supports |
- The degree of reduction can be assessed – it might be possible to reduce rotation to neutral immediately or it might require a gradual approach due to, for example, experienced pain. Therefore, a configurable and adjustable back support can respond to these gradual changes in a clinically appropriate manner.
- For a gradual change, padding can be provided behind the side of the pelvis that is rotated forward, but still allow the pelvis to immerse into the back rest as rotation is reduced over time. These pads can be removed until the pelvis is in a neutral alignment.
- The contouring of the back support behind the PSIS can be maintained on the side that is rotated backwards to ‘block’ further rotation. An adjustable back support can effect direct change to pelvic rotation, and in conjunction with contoured cushion and anterior pelvic support device selection can offer optimal positioning and stability.
- Simultaneous contouring around the waist or lower thoracic region to provide posterior and lateral support, specific to the user’s body shape, can assist to optimise stability in the trunk and reduce the effort of sitting.
- Use of lateral trunk supports can also provide increased trunk stability. Accessories and contouring required will depend on your clinical findings and what is required to block postural asymmetry and reinforce support for stability and function.
 |
 |
Figure 5 & 6 Example of contouring possible within Spex Classic & Spex Supershape back support’s pocket layer for pelvic and trunk asymmetry
The pelvis bears the weight of the upper body in sitting and the ischial tuberosities or ‘sit bones’ are themselves curved leading to greater instability. Failure to adequately support the pelvis with the seat cushion and back support result in posterior pelvic tilt with increased pressure injury risk, trunk lateral flexion and twisting as the upper body seeks to find a stable, supported position to enable functional movement of the arms and head.
A configurable, contourable and adaptable back support allows for optimal support, stability, and pressure-distribution to facilitate preservation/restoration of body shape in sitting, meeting both clinical and functional needs.
How easy have you found it to adjust contouring in the back support to respond to asymmetry in the transverse plane of motion (rotation)?
We will be exploring how back supports can be better contoured to respond to asymmetry in the sagittal plane, namely with pelvic anterior and posterior tilt, in Part 2 of this blog.
Thank you for reading!
- Babinec, M., Cole, E., Crane, B., Dahling, S., Freney, D., Jungbluth-Jermyn, B., Lange, M. L., Pau-Lee, Y.-Y., Olson, D. N., Pedersen, J., Potter, C., Savage, D., & Shea, M. (2015). The Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Position on the Application of Wheelchairs, Seating Systems, and Secondary Supports for Positioning Versus Restraint. Assistive Technology, 27(4), 263–271. https://doi.org/10.1080/10400435.2015.1113802
- Costigan, F. A., & Light, J. (2011). Functional Seating for School-Age Children With Cerebral Palsy: An Evidence-Based Tutorial. Language Speech and Hearing Services in Schools, 42(2), 223. https://doi.org/10.1044/0161-1461(2010/10-0001)
- Kobara, K., Eguchi, A., Watanabe, S., & Shinkoda, K. (2008). The influence of the distance between the backrest of a chair and the position of the pelvis on the maximum pressure on the ischium and estimated shear force. Disability and Rehabilitation. Assistive Technology, 3(5), 285–291. https://doi.org/10.1080/17483100802145332
- Minkel, J. L. (2018). Seating and mobility evaluations for person with long-term disabilities: Focusing on the client assessment. In Seating and Wheeled Mobility: A clinical resource guide (pp. 3–26). Slack Incorporated.
- O’Sullivan, S. B., Schmitz, T. J., & Fulk, G. (2019). Physical Rehabilitation (7th ed.). F.A. Davis.
- Samuelsson, K., Bjӧrk, M., Erdugan, A.-M., Hansson, A.-K., & Rustner, B. (2009). The effect of shaped wheelchair cushion and lumbar supports on under-seat pressure, comfort and pelvic rotation. Disability & Rehabilitation: Assistive Technology, 4(5), 329–336.
- Sprigle, S., Wootten, M., Sawacha, Z., Thielman, G., & Theilman, G. (2003). Relationships among cushion type, backrest height, seated posture, and reach of wheelchair users with spinal cord injury. The Journal of Spinal Cord Medicine, 26(3), 236–243. https://doi.org/10.1080/10790268.2003.11753690