


This blog aims to provide some guidance on the potential causes and presentation of anterior pelvic tilt for wheelchair users. Seating solutions such as belts, back supports, chest straps and harnesses will be considered along with how Spex cushions can help to manage outcomes for functional seating.
Pelvic tilt affects how the upper body is stacked above the pelvis. A neutral pelvic tilt means that the normal curvatures of the spine are maintained, and this reduces the physical effort and adaptation our bodies perform to maintain balance and equilibrium – we do not have to work quite so hard if this is symmetrical and stable. Think about the difference in effort you might experience standing on your whole foot to then standing on your tip-toes.
Simply put, anterior pelvic tilt means that the pelvis rolls forward, increasing the lumbar lordosis curve.

Figure 1: Example of mild anterior pelvic tilt presentation in sitting
In lying this may be easily discovered by an increase in the space between the lumbar curve (Figure 2: see the blue arrows below) and the supporting surface.
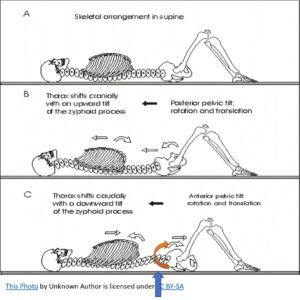
Figure 2: Picture C = presentation of anterior pelvic tilt in lying
In medical terms, anterior pelvic tilt is described as a forward rotation of the pelvis in the sagittal plane around the Z axis (Figure 3). This results in the anterior superior iliac spine (ASIS) of the pelvis rotating forward so that it becomes lower in comparison to the posterior superior iliac spine (PSIS) of the pelvis – these are the bony landmarks we feel when we do a clinical assessment of posture.
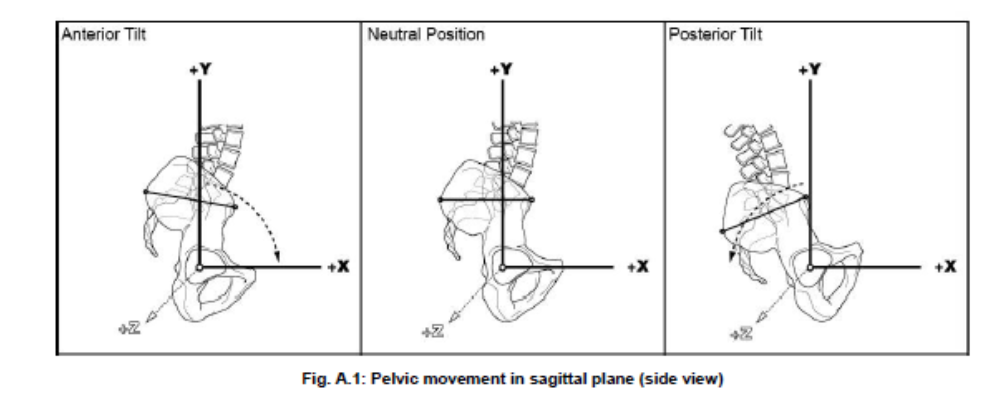
Figure 3: Pelvic movement in the sagittal plane (Waugh & Crane, 2013, p. 309)
Anterior pelvic tilt increases the lumbar lordosis and may result in a flattened thoracic kyphotic curve even with potential arching of the back (trunk extension) and/or neck extension as the person adjusts the trunk and head position to optimise balance and efficiency against the force of gravity pushing down when sitting. Severe anterior tilt when sitting on a flat surface may result in an individual not being able to use their hands, as they might require one or both hands to prop in order to maintain the weight of the upper body now leaning forward over the pelvis and no longer in contact with the back support. Therefore, function becomes severely limited as the wheelchair user cannot use their hands without losing sitting balance. This can lead to further long-term postural changes if the seating system (cushion, back support, arm rests, and so forth) does not offer appropriate support to effectively reduce or accommodate seating effort or asymmetry.
1. Where some, but not full reduction in asymmetry is possible beacuse of tight hip flexors, a Spex cushion can be used to provide initial ramping (front higher than the back) that can be gradually reduced as tolerance allows.
 |
 |
Figure 4: The Spex cushion can allow for adjustment towards a more neutral pelvic tilt by adjusting the pocket layer contouring.
If the Spex cushion is used to respond to reducible anterior pelvic tilt the contouring chart may look like this above to start with, then the number of pads along the length of the thigh could be gradually reduced until the wheelchair user can comfortably sit on a level seating surface and maintain contact through the back support. Care must be taken that:
- The feet are well supported on the foot supports to relieve potential pressure under the front of the thighs on the cushion edge,
- The arm rests are adjusted for comfort,
- Pressure and skin integrity is closely monitored,
- The back support offers adequate support and immersion for stability, and
- Functional goals are evaluated when in this position.
2. We can use support in the opposite direction to the rotation at the level of the ASISs by, for example, using an anterior pelvic support (belt). This provides a biomechanical block to the pelvis rotating forwards and can help offer stability. A pelvic belt may have a perceived stigma attached by the wheelchair user and/or caregivers and therefore it is critical that its role is understood.
 |
 |
Figure 5: The direction of force considered for anterior pelvic support and an example of support available.
3. If a more rigid pelvic stabiliser is required, such as used by Ryan et al. (2005) with children with Cerebral Palsy, this can be created using Spex extended lateral brackets and a swing away lateral support pad to place a rigid block in front of either side of the pelvis.
4. The pelvis and trunk both need to be well supported on the cushion and back support. Consider the contact and contouring required for stability.
A key focus will be in helping to orientate the pelvis so that the spine and head are stacked vertically above the pelvis and to allow the wheelchair user’s back to be in contact with the back support to optimise comfort, stability and reduced sitting effort.
This may require various approaches, which may be used simultaneously:
1. Angling the seat so that the knees are higher than the hips (accommodating hip flexion) so that the pelvis can move into a neutral tilt with the back against the back rest. This can be accomplished with the Spex cushion (up to around 95° hip flexion), the Spex Flex cushion (up to 110° hip flexion), or by using a foam wedge under the cushion to add contouring to better align the pelvis. Please note this will increase the pressure loading on the ischial tuberosities and sacrum which warrants careful analysis and evaluation.
Figure 6: Example of backward angled (ramped) seat where knees are higher than the hips (Engstrom, 2011)
 |
 |
Figure 7: The Spex Flex cushion can respond to bilateral and unilateral (shown above) hip flexion limitations that influence pelvic tilt, rotation and obliquity.
You may find that there are tight hip flexors on one side of the pelvis (unilateral). The Spex Flex cushion is designed to accomodate and respond to hip flexion asymmetry between 70°-110° allowing simple adjustment, where possible.
2. Ensuring that the back rest is sufficiently supportive and if necessary, contourable, to provide additional support behind the pelvis and the user’s back without pushing the trink forward. This will improve stability and comfort. The height of the trunk depends on the functional and stability needs of the wheelchair user. Full back supports, like the Spex or Spex Supershape back supports allow for varying contouring that facilitates immersion and reinforced support for comfort.
 |
 |
 |
Figure 8: Spex (left), TSS (middle) and Spex Supershape (right) offer contouring through their configuration for immersion.

Figure 9: Spex Supershape contouring to illustrate ability to respond to increased lumbar lordosis whilst maintaining contact with the wheelchair user’s full back.
3. Utilising wheelchair tilt, to bring the trunk vertical againist gravity (if starting position is with trunk forward of pelvis). This needs to be carefully considered if the client presents with neck movement limitations preventing them from being able look around easily when in a tilted position.
4. An anterior trunk support (e.g. a chest strap or harness) may help provide support to the front of the chest, reducing the trunk falling forward over the thighs, whilst allowing free movement of the hands. This, however, requires careful consideration for individuals with breathing difficulties where compression on the chest from the force of the forward leaning may reduce respiratory efficiency. An anterior chest support should also avoid the percutaneous endoscopic gastronomy (PEG) tube side, if applicable. Chest straps need to be understood as a postural support device rather than a restraint (Babinec, 2015) and acceptable for the wheelchair user and caregivers, without causing discomfort.
 |
 |
Figure 10: Example of anterior chest supports.
5. A tray on the wheelchair can provide additional support to the forearms to allow weight-bearing and stability if the trunk is forward of the pelvis.
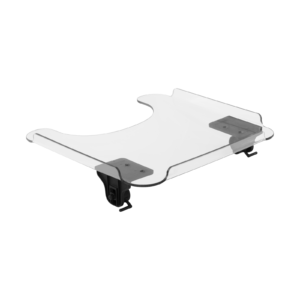
Figure 11: Spex Tray table with slide and lock hardware
6. Adjustable arm supports can optimise the angle and level beneath the forearms for stability. In combination with tray table they assist to improve upper body stability essential to accomplishing tasks.

Figure 12: Spex angle-adjustable arm support
Modular seating technology can be effective at responding to anterior pelvic tilt. Components need to be matched to functional goals, postural need and personal preferences. Secondary postural deviations in response to anterior pelvic tilt may become non-reducible/permanent over the long-term if not adequately addressed.
The seat cushion and back support (height and contact area against the body) play a crucial part in providing the primary functional seating surfaces for stability. Secondary supports and accessories are an essential consideration for reinforcing support against gravity and reducing the effort of sitting, whilst also facilitating easy transfers in and out of the wheelchair and caregiver access when required.
Thank you for reading!