

This article is a simple refresher to pelvic anatomy, what we mean by ‘stability’ and how we can optimise this in wheelchair sitting. Clinical evidence to support this blog is listed at the end.
There are key pelvic landmarks we refer to during assessments for wheelchair seating.
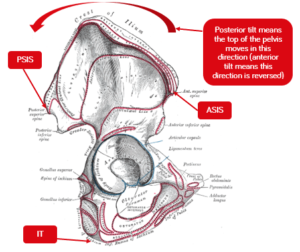
- Anterior superior iliac spine (ASIS) which are the top front points of the hip bones when resting your hands on your hips,
- Posterior superior iliac spine (PSIS) often marked by dimples or indents on our lower back where the PSIS are close to the skin, and
- Ischial tuberosities (ITs) which are the sharp points you feel when sitting on a hard surface
 |
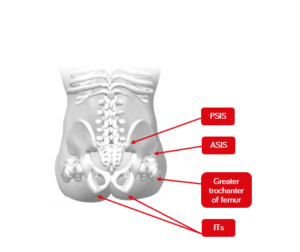 |
| Figure 1. Lateral view of the pelvis | Figure 2. Posterior view of pelvis in sitting |
{kind=link}
We are concerned with whether these landmarks are in an anatomically ‘neutral’ position meaning that the pelvis isn’t twisted with one side more forward than the other (pelvic rotation), lower on one side (pelvic obliquity) or angled forward/backward when looking at the side-view of the pelvis (anterior/posterior pelvic tilt) and creating secondary complications to the spinal alignment. A neutral sitting position also refers to the correct alignment of the spine, head, and neck in relation to the spine and where the line of gravity falls over the pelvis (Neville, 2005).
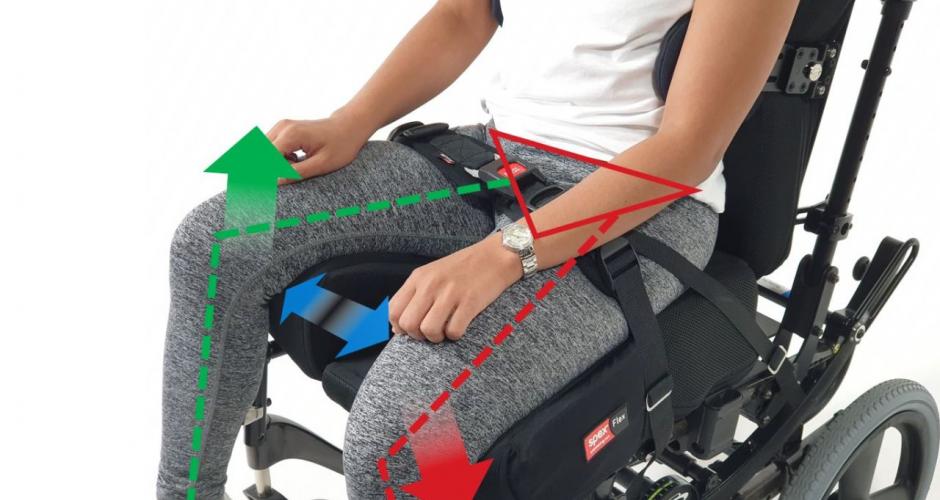
The anatomical shape of the ITs is curved (see Figure 2 above), and this can create pelvic instability as there is no flat surface on which to balance. Also the pelvis tends to tilt a little![]() backwards in sitting and, although this may provide for added stability when reaching (Sprigle et al., 2003) the normal curves of the spine need to be maintained – if the pelvis is too forward on the seat in relation to the back rest (contributing to posterior pelvic tilt) or if it tilts too far backwards (increasing posterior tilt) this can increase the risk of developing decubitus pressure ulcers (Kobara et al., 2008) and result in hyper kyphosis and loss of the lumbar curve (see Figure 3). We need to optimise the tilt of the pelvis to alleviate the risk of pressure area development and secondary spinal deformities, and we need to control rotation and obliquity for a good sitting posture (Samuelsson et al., 2009).
backwards in sitting and, although this may provide for added stability when reaching (Sprigle et al., 2003) the normal curves of the spine need to be maintained – if the pelvis is too forward on the seat in relation to the back rest (contributing to posterior pelvic tilt) or if it tilts too far backwards (increasing posterior tilt) this can increase the risk of developing decubitus pressure ulcers (Kobara et al., 2008) and result in hyper kyphosis and loss of the lumbar curve (see Figure 3). We need to optimise the tilt of the pelvis to alleviate the risk of pressure area development and secondary spinal deformities, and we need to control rotation and obliquity for a good sitting posture (Samuelsson et al., 2009).
Figure 3. Example of posterior tilt of the pelvis and contribution to hyper-kyphosis
Essentially what we aim for is:
- ITs to be level on the seat
- Pressure loading to be shared across ITs, greater trochanters, and posterior superior iliac spines
- Pressure loading also be taken through the back of the thighs (in a manner that doesn’t pull the pelvis forward or cause the pelvis to tilt backwards/forward), arms, back, feet and head (if required) to optimise comfort
- Pelvic rotation, posterior tilt, and obliquity to be controlled or minimised to prevent secondary postural asymmetry, and
- Provide a stable seated foundation that the spine, shoulders, head, and neck can be aligned above the pelvis with the line of gravity falling through the centre of the pelvis and the anatomically neutral curves of the spine maintained.
The human body is inherently unstable – our body parts move independently to one another and our central anchors of pelvis and spine and shoulders can move in multiple directions in relation to each other. If the body’s neurological system is affected (sensory loss, muscle tone changes, muscle weakness, impaired coordination) and muscles can no longer support a neutral alignment, then these joints become even more unstable and this affects the functional ability to use our arms and legs and head freely. The human body is amazing and complex.
Stability refers to the energy or effort required to create imbalance, where our line of gravity falls outside of our base of support. Person A (below) is stable, person B is less stable as the line of gravity is now at the front of his base of support. To make himself more stable, person C simply needs to step forward and lower the load, so that the line of gravity again falls within the centre of the base of support.
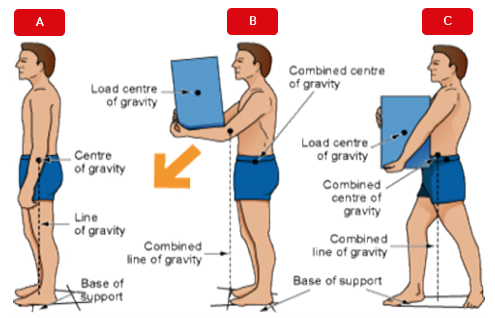
This Photo by Unknown Author is licensed under CC BY
Our base of support in standing is created by our feet, which have the only contact with the supporting surface. Of course, high heels reduce the contact we have with the supporting surface, move our line of gravity forward in relation to our base of support and raise our centre of gravity, making us less stable – less energy would be required to knock one over compared to if one was wearing flat shoes.
Sitting can be less stable than standing because of the curved shape of the ITs now bearing most of the upper body weight, and the potential for rotation, obliquity and tilt based on our sitting posture on the seating surfaces. Instability can also be inherent because of changes to one’s musculoskeletal and neurological systems affecting the positioning of the pelvic, which is the “keystone” (Pope, 2007) of posture.
Now let us consider the pelvis anatomical position and its effect on stability:
- Pelvic obliquity – one side is lower than the other meaning that most of the body weight is on one IT and the upper body must balance on a smaller bony surface. This creates a knock-on effect on the spine and the hip joints which will adjust their position to regain that stability and, potentially, to offload increased pressure. This can effectively contribute to twisting in the spine and trunk (scoliosis), changes in hip joint position (hip flexion asymmetry) and require more effort and energy to maintain sitting posture.
- Pelvic rotation – if the pelvis is level but rotated, weight is still transferred across both ITs, but rotation can cause the spine to twist which makes sitting more effortful.
- Pelvic tilt – tilt either forwards or backwards requires the muscles to hold the position and again make sitting more effortful. This affects the curves of the spines. Pelvic position, which affects posture of the upper body, can affect vital functions, like breathing, and movement of the upper extremities.
Failing to create pelvic stability (by reducing/stabilising presenting postural asymmetry) means pressure distribution can contribute to skin integrity risks, sitting becomes effortful, function of the arms and head potentially more difficult and secondary complications of postural alignment can develop or become exacerbated. The pelvis position can affect vital functions such as breathing (Lin et al., 2006), reaching ability (Samuelsson et al., 2003; Myhre & von Wendt, 1991) and therefore stability and function in sitting need to be simultaneously considered.
When the pelvis can be reduced towards a more neutral alignment because of joint flexibility, then this will be the primary goal. When this is not possible or limited, the supporting surfaces need to be adjusted to accommodate the asymmetry and provide the necessary reinforcing support to optimise alignment and provide support. The first step is always to complete a thorough assessment of someone’s posture to see where there are limitations in movement (non-reducible) and where asymmetry is reducible (flexible) to achieve a more neutral pelvis position:
a) Consider the type of wheelchair
Wheelchairs needs to be configured to allow stability and function as well as to allow ways to reduce pressure during seating posture (e.g. through tilt). Sling or canvas wheelchairs are perhaps the most common wheelchair prescribed; however, these can encourage the pelvis into posterior tilt (Amos et al., 2001) and can also create obliquity if the pelvis is not aligned at the centre of the seat. The shape of the spine should be maintained to optimise sitting posture (Lange & Minkel 2018; Amos et al., 1991) and this means avoiding posterior and anterior pelvic tilt which can flatten the curves of the spine and cause twisting – both of these affect postural stability. The seat and back rest can contribute to asymmetry if surfaces do not optimise neutral alignment.
A generic wheelchair may not be correctly sized or set up for the wheelchair-user’s unique shape and postural needs and therefore careful consideration of the type of wheelchair and supporting surfaces and accessories is required. If the wheelchair size is too big (or small) for a wheelchair-user, this can result in secondary postural deformities developing due to inadequate support or by the wheelchair-user adopting a position that is, perhaps, more comfortable. Correct sizing of the wheelchair is vital and needs to include seat width, seat depth, back rest height, arm rest height and footrest height.
Configurability of the wheelchair is also important as the seating system may need adjustments over time to respond to postural changes of the wheelchair-user and changes in, for example, transfer ability.
b) Adapt the supporting cushion surface to optimise comfort, pressure distribution and shaping to create a stable base of support.
Cushion selection needs to be considered in the context of shape, pressure relieving properties, and adjustment and customisations required and whether these match the clinical and postural needs of the wheelchair-user. We can do a variety of things to provide stability to the pelvis:
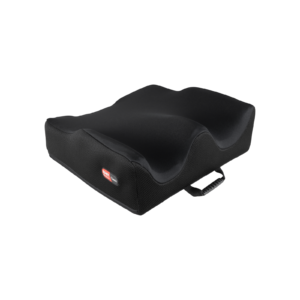
- Provide a more contoured surface that provides shaping under the ITs and contouring around the thighs, provides a greater surface area to support the pelvis and thighs, in addition to redistributing pressure to offload the ITs to promote comfort. Shaping in the cushion, with additional support from a lumbar support, can also support the pelvis toward a more neutral position (Samuelsson et al., 2009). The back support lowest height, if positioned at the level of the PSIS and against the body, can be used to help orientate and stabilise the pelvis.
 |
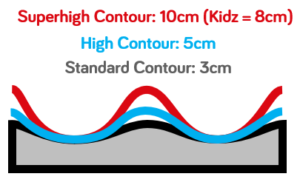 |
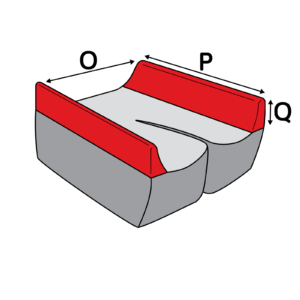
Figure 4. Example of cushion contouring around the pelvis and thighs with variations to meet clinical need
- Ensure that when the cushion is removed for hygiene care it is replaced into the correct position on the seat pan and secure (often Velcro is used to secure cushions on the seat pan) with the covers on correctly (for pressure management and hygiene needs).
- Ensure that the cushion cover has sufficient stretch to allow the pelvis to be immersed into the cushion shape and meet the supporting surface.
- Adjust the support underneath the ITs to ensure that weight is taken as equally as possibly by both ITs by building up support to encourage a reducible obliquity (i.e. this is flexible) or by building up support to stabilise a non-reducible obliquity – failure to do this will likely result in the upper body flexing to find a ‘balancing point’ where stability is maintained and cause further trunk asymmetry and postural deformity.
 |
 |
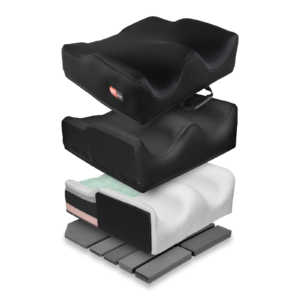
Figure 5. Example of cushions (Spex Classic & Spex Flex) that allow adjustment to meet pelvic and hip asymmetry and various foam and cover configurations. Cushions may have additional customisations relating to foam used or shaping.
- Adjust the type of material under the ITs to provide increased stability. When talking about products, ‘stability’ can mean firmness (O’Sullivan, Schmitz& Fulk, 2019, p. 1402) but this must be considered in conjunction with skin integrity needs as softer materials or different types of cushions may be required to respond to and maintain skin integrity for wheelchair-users at high risk of pressure ulcer development. This can also be managed by establishing a regime to relieve pressure through use of wheelchair features (e.g. tilt) or by the wheelchair-user/caregivers adjusting pressure distribution through transfers. Customisations of cushion are also possible to meet individual need.
- Provide a pre-ischial shelf in the cushion to provide a well for the ITs to rest and be supported, maintain neutral pelvic alignment, and reduce sliding forward on the seat. This can be adjusted according to individual need in conjunction with pressure management needs.
 |
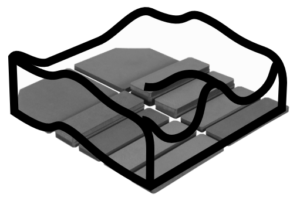 |
Figure 6. Spex Cushion configuration in response to posterior pelvic tilt or extensor thrust
- Build up or reduce the height of the support under the thighs to reduce/accommodate hip flexion asymmetry or manage tone contributing to pain or changes to the pelvis position in sitting so as to prevent secondary postural distortions this can create (Ágústsson et al., 2017).
 |
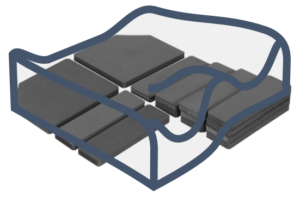 |
Figure 7. Example of Spex classic cushion configuration for mild hip flexion asymmetry
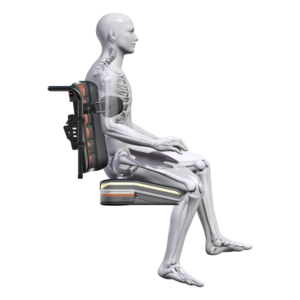
Figure 8 Spex Flex cushion configurations for moderate hip flexion asymmetry considering back support and trunk accessories
- Increase support laterally (on the sides) of the pelvis by adding additional shaping and contouring around the pelvis. Where an anterior support belt is used, the lateral support to the pelvis may need to allow correct positioning of the belt so that it maintains the needed contact with the pelvis.
 |
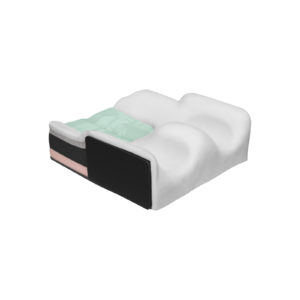 |
Figure 9. Example of adjusting lateral pelvic support (left) and considering this when used with anterior pelvic positioning belt

Figure 10. Example of hip/thigh lateral supports
c) Provide additional support with accessories to support the pelvis
Accessories such as harnesses, straps or belts can be met with unease due to concerns that these are restraints. Babinec et al. (2015) explains this well:
“Practitioners usually refer to these devices as “supports” rather than “restraints,” for two reasons:
- “Supports” are used to achieve a very specific position or posture of a body part in addition to minimizing migration in a specific direction.
- “Restraints” typically refer to devices that are used to limit harmful motion during vehicular transportation, or a device that is carefully controlled in many settings.”
Pelvic supports can include 2- or 4-point pelvic belts and anterior/ lateral hip pads, which can block or minimise the pelvis movement into obliquity, rotation, or tilt. They can also include supports at the knee to provide support in the presence of tone or neuromotor disturbances to maintain the hip alignment and prevent changes to pelvic position in sitting.
 |
 |
Figure 11. Example of 2-point (left) and 4-point (right) pelvic support belt
d) Optimise the position of the secondary supporting surfaces to the body
Foot supports, arm supports, lateral trunk supports, and head supports are intended to optimise sitting position, offload pressure to maintain skin integrity and comfort, and support the optimal pelvic position on the seating surface. Where there is pelvic asymmetry that needs to be accommodated, these supporting surfaces provide reinforcing support to the body segments to maintain sitting posture and stability and facilitate the body’s ability to engage in functional activities.

Figure 12. The full seating system needs to consider the cushion, back support, arm supports, lateral trunk supports, head supports and foot supports and accessories (not shown above) to optimise sitting posture and postural control for function
- Ágústsson, A., Sveinsson, Þ., & Rodby-Bousquet, E. (2017). The effect of asymmetrical limited hip flexion on seating posture, scoliosis and windswept hip distortion. Research in Developmental Disabilities, 71, 18–23. https://doi.org/10.1016/j.ridd.2017.09.019
- Amos L, Brimner A, Dierckman H, Easton H, Grimes H, Kain J, Bednarski J, & Moyers PA. (2001). Effects of positioning on functional reach. Physical & Occupational Therapy in Geriatrics, 20(1), 59–72.
- Babinec, M., Cole, E., Crane, B., Dahling, S., Freney, D., Jungbluth-Jermyn, B., Lange, M. L., Pau-Lee, Y.-Y., Olson, D. N., Pedersen, J., Potter, C., Savage, D., & Shea, M. (2015). The Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Position on the Application of Wheelchairs, Seating Systems, and Secondary Supports for Positioning Versus Restraint. Assistive Technology, 27(4), 263–271. https://doi.org/10.1080/10400435.2015.1113802
- Kobara, K., Eguchi, A., Watanabe, S., & Shinkoda, K. (2008). The influence of the distance between the backrest of a chair and the position of the pelvis on the maximum pressure on the ischium and estimated shear force. Disability and Rehabilitation. Assistive Technology, 3(5), 285–291. https://doi.org/10.1080/17483100802145332
- Lange, M., & Minkel, J. (2018). Seating and Wheeled Mobility: A Clinical Resource Guide. Slack Incorporated.
- Myhr, U., & von Wendt, L. (1991). Improvement of functional sitting position for children with cerebral palsy. Developmental Medicine and Child Neurology, 33(3), 246–256. https://doi.org/10.1111/j.1469-8749.1991.tb05114.x
- Neville, L. (2005). The Fundamental Principles of Seating and Positioning in Children and Young People with Physical Disabilities. University of Ulster.
- O’Sullivan, S. B., Schmitz, T. J., & Fulk, G. (2019). Physical Rehabilitation (7th ed.). F.A. Davis.
- Pope, P. (2007). Severe and Complex Neurological Disability. Elsevier. https://doi.org/10.1016/B978-0-7506-8825-3.X5001-5
- Samuelsson, K., Bjӧrk, M., Erdugan, A.-M., Hansson, A.-K., & Rustner, B. (2009). The effect of shaped wheelchair cushion and lumbar supports on under-seat pressure, comfort, and pelvic rotation. Disability & Rehabilitation: Assistive Technology, 4(5), 329–336.
- Sprigle, S., Wootten, M., Sawacha, Z., Thielman, G., & Theilman, G. (2003). Relationships among cushion type, backrest height, seated posture, and reach of wheelchair users with spinal cord injury. The Journal of Spinal Cord Medicine, 26(3), 236–243. https://doi.org/10.1080/10790268.2003.11753690